The countries of the Americas are today grappling with many of the same fundamental health challenges that gave rise 30 years ago to Alma Ata’s call for “Health for All by the Year 2000.” Despite impressive gains in life expectancy and other aggregate indicators, millions of people still lack access to health care and other conditions essential for good health. Health systems are plagued by high costs and inefficiencies and have had difficulty responding to major changes in epidemiologic and demographic trends. National health budgets are perpetually underfunded despite widespread acceptance of Alma Ata’s message that promoting and protecting health is essential to sustained economic and social development and good quality of life.
Over the past three decades, many countries have tried to tackle these problems through health system reform, but their efforts have had limited, mixed, and even counterproductive results. Health sector reforms of the 1980s and 1990s sought to improve cost-effectiveness and financial sustainability through decentralization, deregulation, and competition but left health systems segmented and fragmented, providing different kinds of care to different groups with little coordination, continuity, or equity. Even efforts to implement primary health care have often failed to produce the desired results. Many countries have applied the approach only selectively, using a handful of high-impact interventions for specific groups or diseases or offering basic, low-cost care for the poor. Only a handful of countries in the Region (including Canada, Chile, Costa Rica, and Cuba, among others) have traditionally made primary health care a pillar of their health systems. They are among the countries that have achieved the best health results.
These experiences and others from around the world clearly show that conventional health systems are ill equipped to meet people’s health needs and that the principles and strategies of primary health care offer the greatest potential to improve health outcomes and reduce inequities in health.

In recognition of this, PAHO Member States in 2003-the 25th anniversary of Alma Ata-collectively renewed their commitment to primary health care in a resolution (CD44.R6) that called on PAHO’s Secretariat to take the principles of primary health care into account in all its technical cooperation activities. The countries urged PAHO to promote the approach through training of health workers, support for locally defined models, and evaluation of different systems based on primary health care. They also called on PAHO to promote celebrations and discussions of the Americas’ 25 years of experience with the approach, with an eye to identifying best practices for implementing primary health care–based reforms throughout the Region.
 As part of this process, PAHO and its Member States organized a series of national and international consultations on primary health care that reached out to civil society, governments, nongovernmental organizations, universities, professional associations, other U.N. agencies, and the international community. Based on a draft by the special Working Group on Primary Health Care and input from the 46th Directing Council in September 2005, PAHO produced Renewing Primary Health Care in the Americas, a position paper that redefines the approach and lays out strategic and programmatic orientations for building health systems based on the renewed vision. Over 40,000 copies of the paper, in all four PAHO official languages, were distributed in the Americas and worldwide. In September 2005, PAHO’s 46th Directing Council expressed its support for the new approach in the Regional Declaration on the New Orientations for Primary Health Care (Declaration of Montevideo). It was further endorsed in the final declaration of the international conference Buenos Aires 30/15: from Alma-Ata to the Millennium Declaration (Buenos Aires Declaration) in 2007, in the Iquique Consensus of the 9th Ibero-American Conference of Ministers of Health, in the Health Agenda for the Americas 2008–2017, and at the Fifth Summit of the Americas (Declaration of Commitment of Port of Spain) in April 2009.
As part of this process, PAHO and its Member States organized a series of national and international consultations on primary health care that reached out to civil society, governments, nongovernmental organizations, universities, professional associations, other U.N. agencies, and the international community. Based on a draft by the special Working Group on Primary Health Care and input from the 46th Directing Council in September 2005, PAHO produced Renewing Primary Health Care in the Americas, a position paper that redefines the approach and lays out strategic and programmatic orientations for building health systems based on the renewed vision. Over 40,000 copies of the paper, in all four PAHO official languages, were distributed in the Americas and worldwide. In September 2005, PAHO’s 46th Directing Council expressed its support for the new approach in the Regional Declaration on the New Orientations for Primary Health Care (Declaration of Montevideo). It was further endorsed in the final declaration of the international conference Buenos Aires 30/15: from Alma-Ata to the Millennium Declaration (Buenos Aires Declaration) in 2007, in the Iquique Consensus of the 9th Ibero-American Conference of Ministers of Health, in the Health Agenda for the Americas 2008–2017, and at the Fifth Summit of the Americas (Declaration of Commitment of Port of Spain) in April 2009.
The PAHO/WHO position paper presents accumulated evidence that shows that health systems based on primary health care are more efficient, have lower costs, and achieve higher user satisfaction than systems that are not. Based on experiences with primary health care in the Americas and other regions, and the inability of existing systems to meet current health needs, the report presents a new vision for primary health care–based reform and offers key strategic directions and lines of action for carrying it out.
The new PAHO/WHO vision remains faithful to the spirit of Alma Ata but differs in important ways from many of the approaches to primary health care that have emerged since 1978. It discards the idea of a defined set of health interventions aimed at specific population groups, calling instead for the transformation of the health system as a whole. It embraces equity, solidarity, and people’s right to the highest attainable level of health as guiding principles. But it also emphasizes quality of services and sustainability. It acknowledges the roles of the public, private, and nonprofit sectors in health care as well as the importance of health system functions other than the provision of medical care. It also recognizes that different countries have different needs, levels of resources, administrative capacities, and cultural preferences, so that a one-size-fits-all approach to primary health care is neither possible nor desirable. Instead, it provides guiding principles and essential areas of action for carrying out comprehensive health reform.
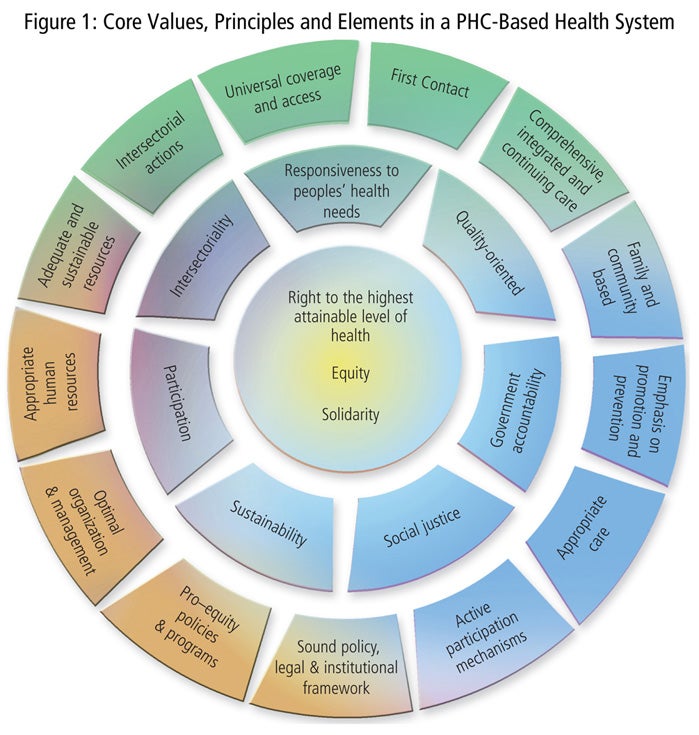
The PAHO/WHO position paper presents three core values, seven principles, and 13 essential elements that are the building blocks of primary health care–based health systems (see Figure 1). Together they create health systems that guarantee universal coverage and access to services that are acceptable to the population and that provide comprehensive, integrated, and appropriate care over time, with an emphasis on prevention and health promotion. They make families and communities the basis for planning and action, and maximize both individual and collective participation in policymaking, prioritizing, and decisions regarding their own health. They promote solidarity, social justice, and equity in access not just to services but to other conditions that are essential for good health.
In 2007, two years after the Declaration of Montevideo, the renewal of primary health care was raised on the global health agenda when the new director-general of WHO, Dr. Margaret Chan, endorsed the approach as “the only way to ensure fair, affordable, and sustainable access to essential care across a population.” A year later, the report of the Commission on Social Determinants of Health provided additional support by documenting the growing gaps in health outcomes within and between countries, analyzing the underlying social, economic, and political causes of these gaps, and citing as one of the best solutions a renewed focus on primary health care.
 Under Dr. Chan’s leadership, WHO carried out its own review of primary health care, drawing on experiences from the Americas and around the globe. This work culminated in the publication of the 2008 World Health Report, Primary Health Care: Now More Than Ever, which presents additional evidence validating primary health care as the best way to ensure equity in health and to equip health systems to meet new challenges. A year later, the 62nd World Health Assembly endorsed the approach and urged its widespread adoption (WHA 62.12 and WHA 62.14).
Under Dr. Chan’s leadership, WHO carried out its own review of primary health care, drawing on experiences from the Americas and around the globe. This work culminated in the publication of the 2008 World Health Report, Primary Health Care: Now More Than Ever, which presents additional evidence validating primary health care as the best way to ensure equity in health and to equip health systems to meet new challenges. A year later, the 62nd World Health Assembly endorsed the approach and urged its widespread adoption (WHA 62.12 and WHA 62.14).
The 2008 World Health Report analyzes major shortcomings that have left conventional health care systems unable to meet the needs of large numbers of people. These include the provision of “inverse care,” whereby better-off people consume more care than people with less means and greater health needs; “impoverishing care,” in which individuals and families who lack social protection fall into poverty as a result of catastrophic out-of-pocket expenses; “fragmented care” due to overspecialization, which prevents a holistic, continuous approach to people’s care; “unsafe care” due to poor system design that fails to ensure safety and hygiene standards; and “misdirected care,” whereby resources are allocated disproportionately toward curative care while neglecting prevention and health promotion.
The report shows that the primary health care approach addresses all these shortcomings by providing clear direction for a comprehensive and balanced response to health needs. It lays out four areas of primary health care–based reform that are critical for building successful health systems:
Universal coverage. To reduce health inequities, all people must have access to health care according to need and regardless of their ability to pay. Countries must undertake reforms and interventions that move them toward universal access and social health protection. These include efforts to expand coverage to the entire population for a growing number of services and with decreasing out-of-pocket costs.
Service delivery. To respond to people’s needs and expectations, health care must be “people-centered.” Countries must undertake efforts to reorganize and reform their health services to ensure continuous, high-quality care that is locally available. This includes efforts to improve both the technical and the perceived quality of health services.
Public policies. Many of the most important determinants of health are beyond the reach of the health sector. Countries must pursue cross-cutting and integrated public policies that encourage prevention and health promotion, and that ensure intersectoral collaboration to address the social determinants of health.
Leadership. Health systems are not evolving on their own toward greater fairness, efficiency and effectiveness. A new direction requires active leadership. Governments must exercise such leadership by facilitating a participatory dialogue that engages all sectors, by building institutional and individual capacities for leadership in health policymaking, and by improving health information gathering to inform the policy debate.
In the Americas, a growing number of countries have embraced the new vision of primary health care and are carrying out initiatives based on these key principles and lines of action. These range from efforts to improve the quality and acceptability of health services to laws and legal frameworks that promote universal health coverage. These include provisions in the new constitutions of Bolivia, Ecuador, and Venezuela that specify health as a basic right of all citizens and assign the State responsibility for guaranteeing inclusion and access to health services (see also Chapter II).
Other major examples of progress toward universal health coverage in recent years include:
Countries of the Region are also making important progress through efforts to better integrate and coordinate their health services, expand access to comprehensive care, encourage prevention and health promotion, and address the social determinants of health. Chapters III through VI of this report highlight a wide range of these efforts in the context of PAHO’s technical cooperation during 2008–2009. Together, these efforts reflect meaningful progress in moving the Region of the Americas closer to its collective goal of “Health for All.”