Part I
A Profile of Adolescents and Youth in the Americas
I.1 Sociodemographic profile of adolescents and youth in the Americas
I.1.1 The adolescent and youth population in the Americas
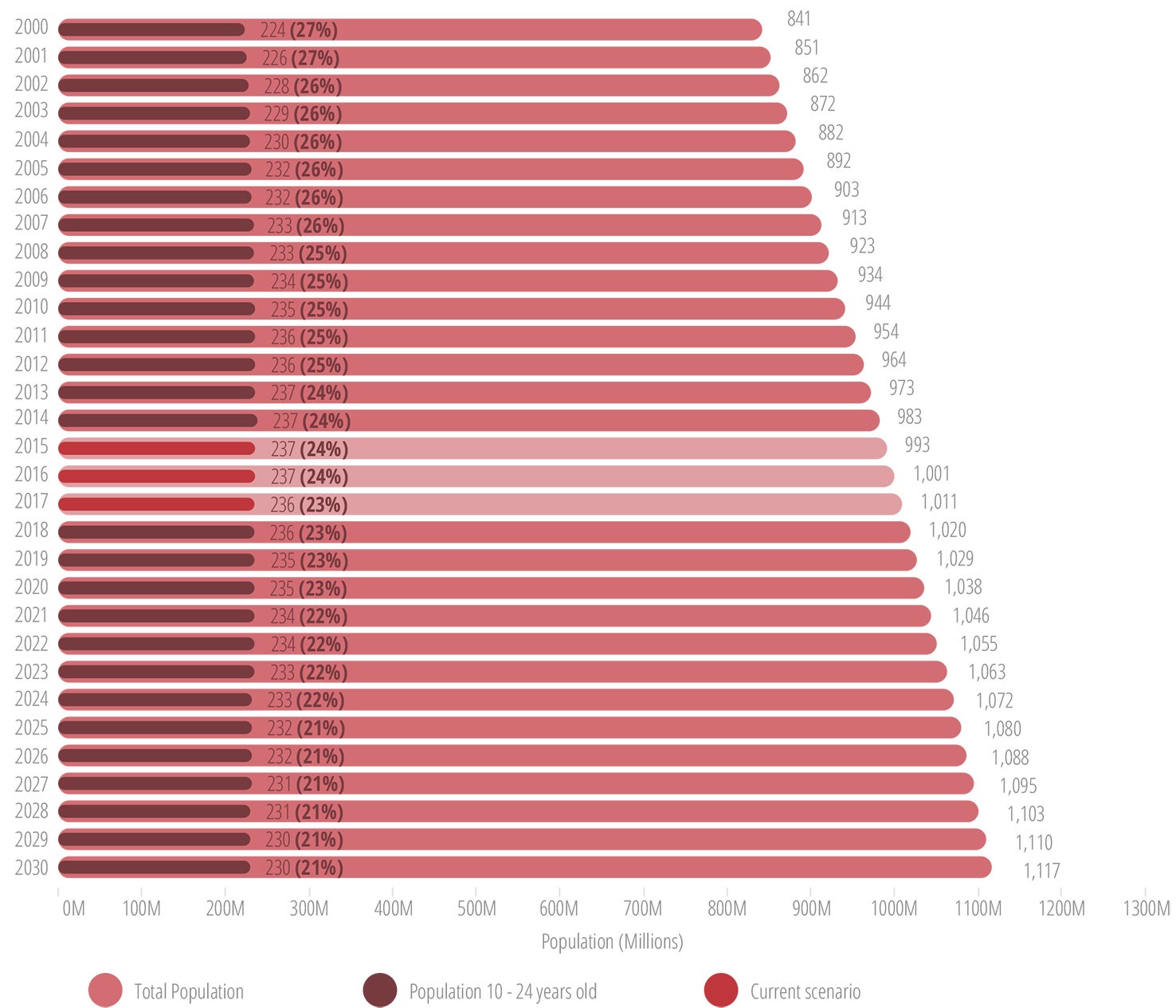
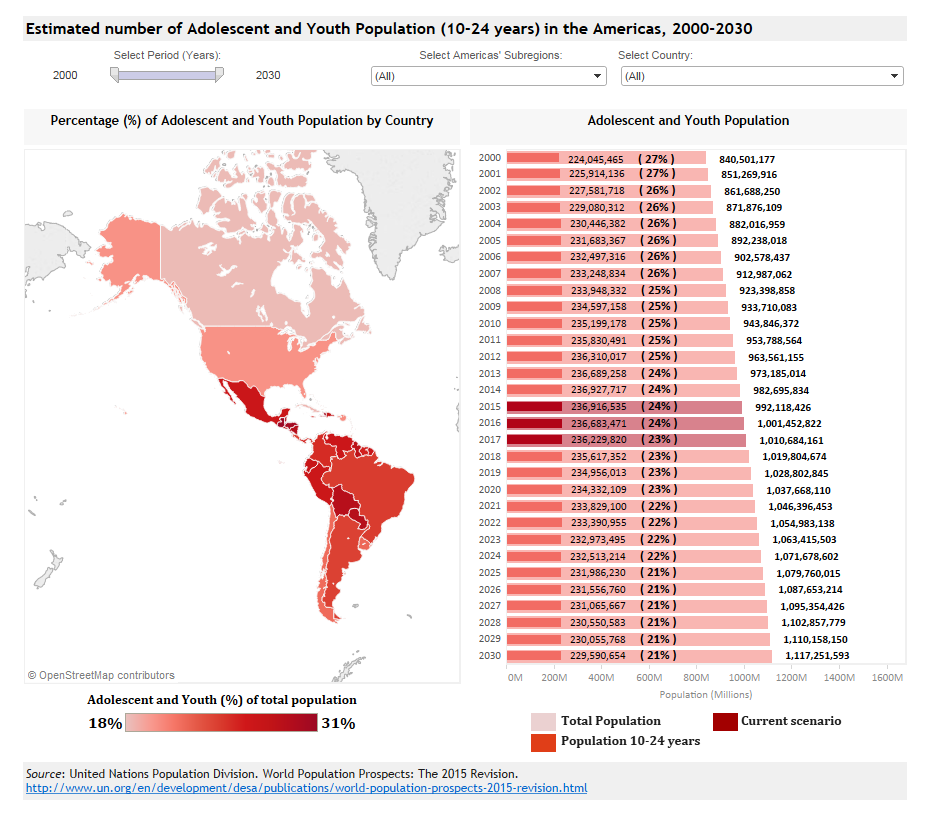
Currently, the population of young people (10-24 years) in the Americas is the largest in the history of the Region, at an estimated 237 million and projected to decrease to 230 million by 2030 (Figure I.1).
Data Visualization
Estimated number of Adolescent and Youth Population (10-24 years) in the Americas, 2000-2030
In 2015, the age group 10-24 constituted 24% of the total population in the Americas and 26% of that in Latin America and the Caribbean (LAC) (Table I.1) (10).
| Total population | Adolescents 10-19 years | Youth 15-24 years | Young persons 10-24 years | ||||
|---|---|---|---|---|---|---|---|
| Number | % | Number | % | Number | % | ||
| The Americas | 992,225,000 | 157,079,000 | 16 | 158,503,000 | 16 | 236,941,000 | 24 |
| North America | 357,838,000 | 45,345,000 | 13 | 48,635,000 | 14 | 71,136,000 | 20 |
| Latin America and the Caribbean | 634,387,000 | 111,734,000 | 18 | 109,868,000 | 17 | 165,805,000 | 26 |
| South America | 418,447,000 | 71,265,000 | 17 | 70,304,000 | 17 | 106,027,000 | 25 |
| Central America | 172,740,000 | 33,229,000 | 19 | 32,390,000 | 19 | 48,984,000 | 28 |
| Caribbean | 43,199,000 | 7,240,000 | 17 | 7,175,000 | 17 | 10,795,000 | 25 |
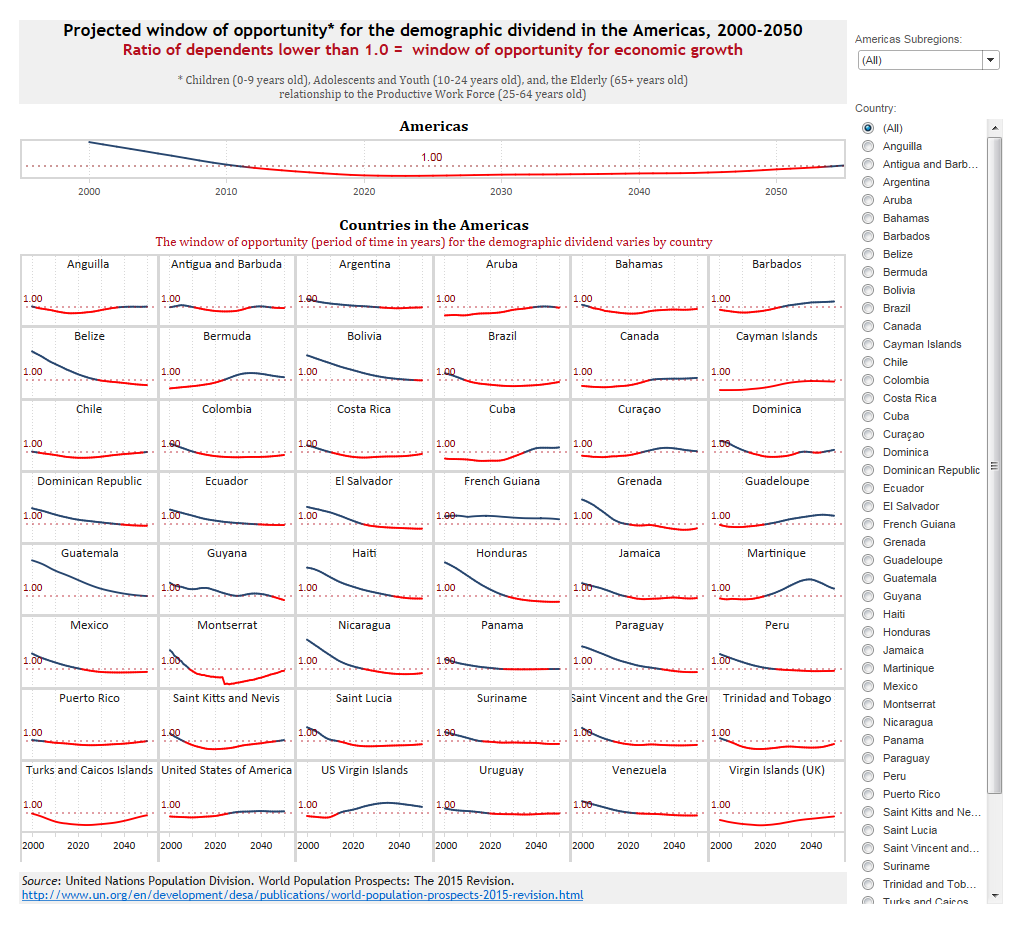
Several countries in the Americas are going through the demographic transition, the shift from high birth and death rates to low fertility, low mortality, and longer life expectancy. The demographic transition is linked to a decline in the ratio of dependents (children and the elderly) to the productive work force, which generates a potential for the “demographic dividend” (10, 11). With fewer people to support, a country has a window of opportunity for rapid economic growth if strategic social and economic policies are developed and investments made (10, 11). The window of opportunity for the demographic dividend varies by country. Most countries are well into the demographic transition, while others are just initiating or have not yet entered into the demographic transition (Figure I.2).
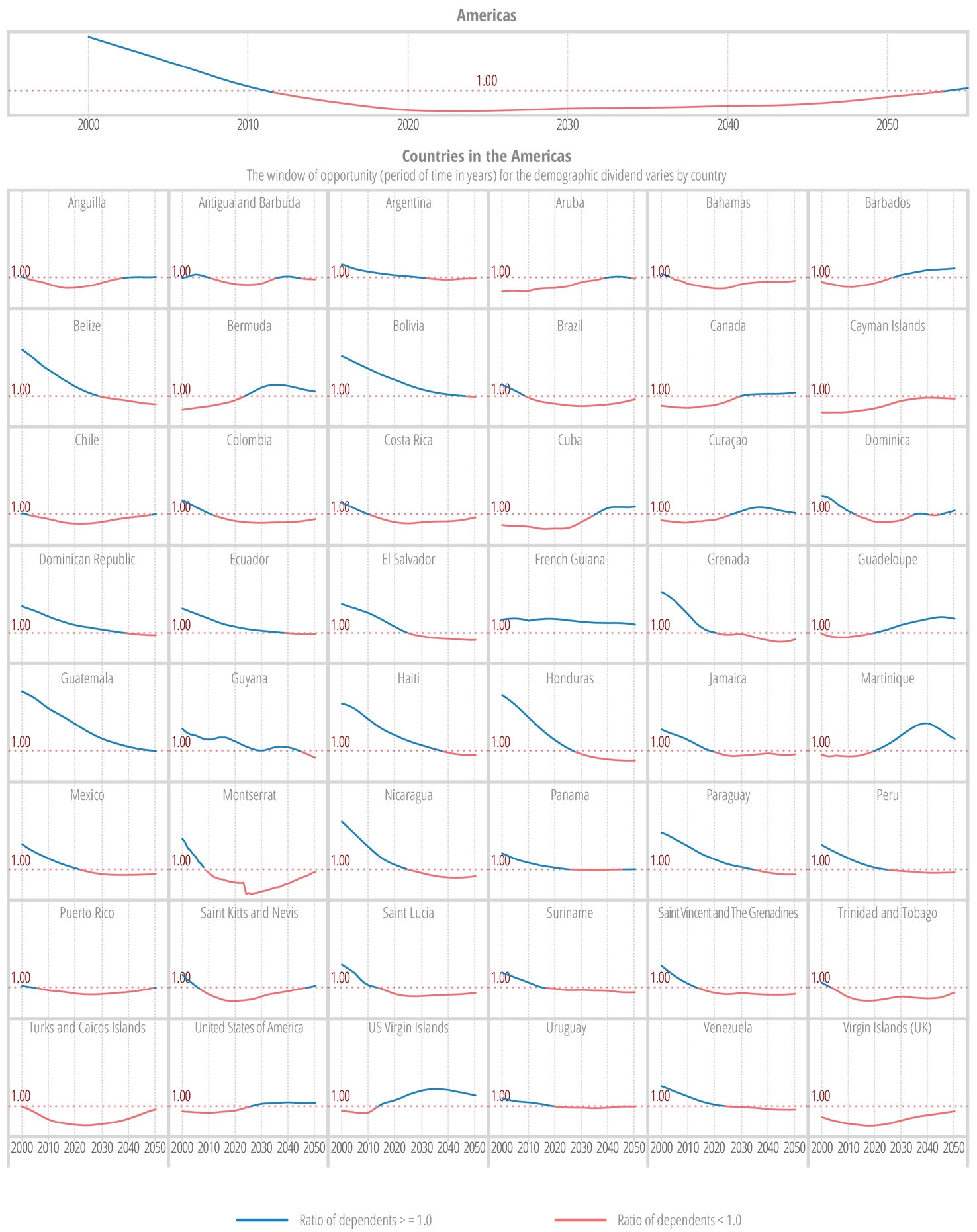
a Ratio of dependents <1.0 is the window of opportunity
Data Visualization
Projected window of opportunity for the demographic dividend in the Americas, 2000-2050

I.1.2 Puberty
The second decade of life is a period of rapid and profound biological, cognitive, emotional, and social development and change. Early adolescence (10-14 years) is characterized by rapid biological transformations for boys and girls, including hormonal changes and the introduction of the capacity to reproduce. Late adolescence (15-19 years) is typified by pubertal maturation and progressive adoption of more adult roles and functions. During adolescence and young adulthood, individuals normally acquire or consolidate the social, cultural, emotional, educational, and economic resources to maintain their health and well-being across the life course (3, 9).
Throughout the life course, the human brain is constantly developing through a process called neuroplasticity. While it was previously thought that the bulk of brain development occurred in the early life years, emerging evidence and understanding in neuroscience suggest that brain functions continue to develop well into adulthood. Research indicates that adolescent brain development is markedly different from brain development in childhood. During childhood the focus is on dendritic outgrowth and synaptogenesis or synaptic growth, allowing the brain to increase significantly in weight and size. In contrast, brain development during the second decade (which continues into early adulthood) appears to focus on synaptic pruning, the process of shedding weak and irrelevant synapses in order to increase the efficiency of the brain. It is believed that synaptic pruning is dependent on the neuron’s responses to environmental factors and external stimuli. This brain development stage characterized by a high rate of synaptic pruning is considered a critical period, where the individual is disproportionately receptive to environmental stimuli. This emerging knowledge explains the adaptive learning and rapid acquisition of interpersonal and emotional skills during adolescence. It also underscores the critical importance of ensuring a secure and stable social environment for adolescents, in order to support optimal development of the brain functions needed for longevity and for social and emotional wellness in adulthood (3, 12, 13).
I.1.3 The social determinants of adolescent and youth health in the Americas
Social determinants of health are the conditions in which people are born, grow, develop, live, work, and age (3, 14, 15). These include structural determinants (such as the socioeconomic and political context, socioeconomic position, gender, ethnicity, education, occupation, and income), as well as intermediary determinants (such as behaviors and biological factors, psychosocial factors, and the health system) (Figure I.3) (15, 16).
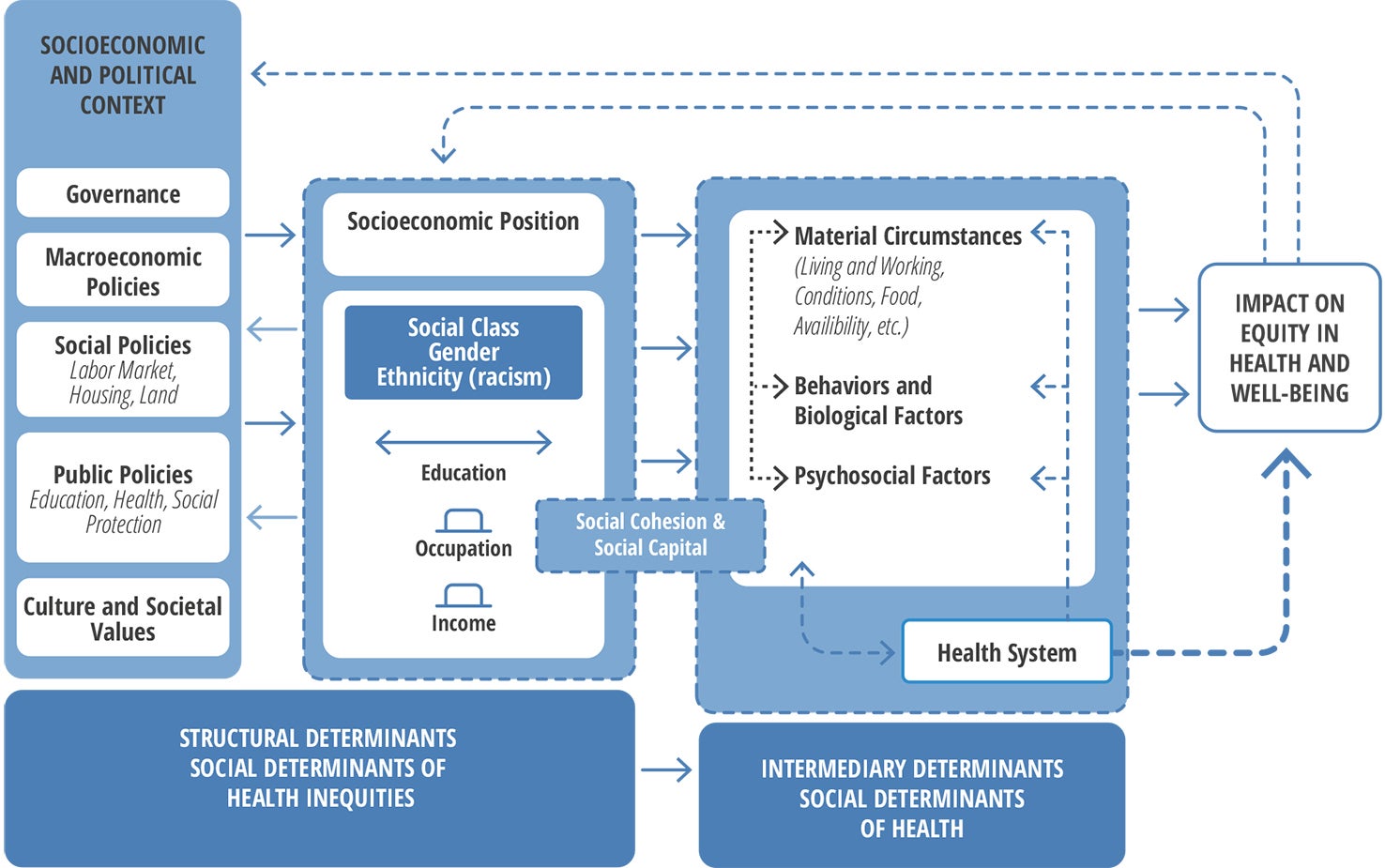
An analysis of the social determinants of health and adolescence identified national wealth, income inequality, and access to education as the strongest determinants of adolescent health (16). In addition, safe and supportive families and schools, and positive and supportive peers were highlighted as crucial to helping young people develop to their full potential and attain the best health in the transition to adulthood (16).
The following paragraphs elaborate on selected determinants, including education, employment, poverty, ethnicity, gender family, peers and media in relation to the health of adolescents and youth.
Education
The level of education is one of the most important determinants of opportunities for employment, income, and health. Education beyond the primary level has been associated with health benefits across the life course, including lower male injury mortality, lower female fertility, improved adult health, and increased survival of future children (16).
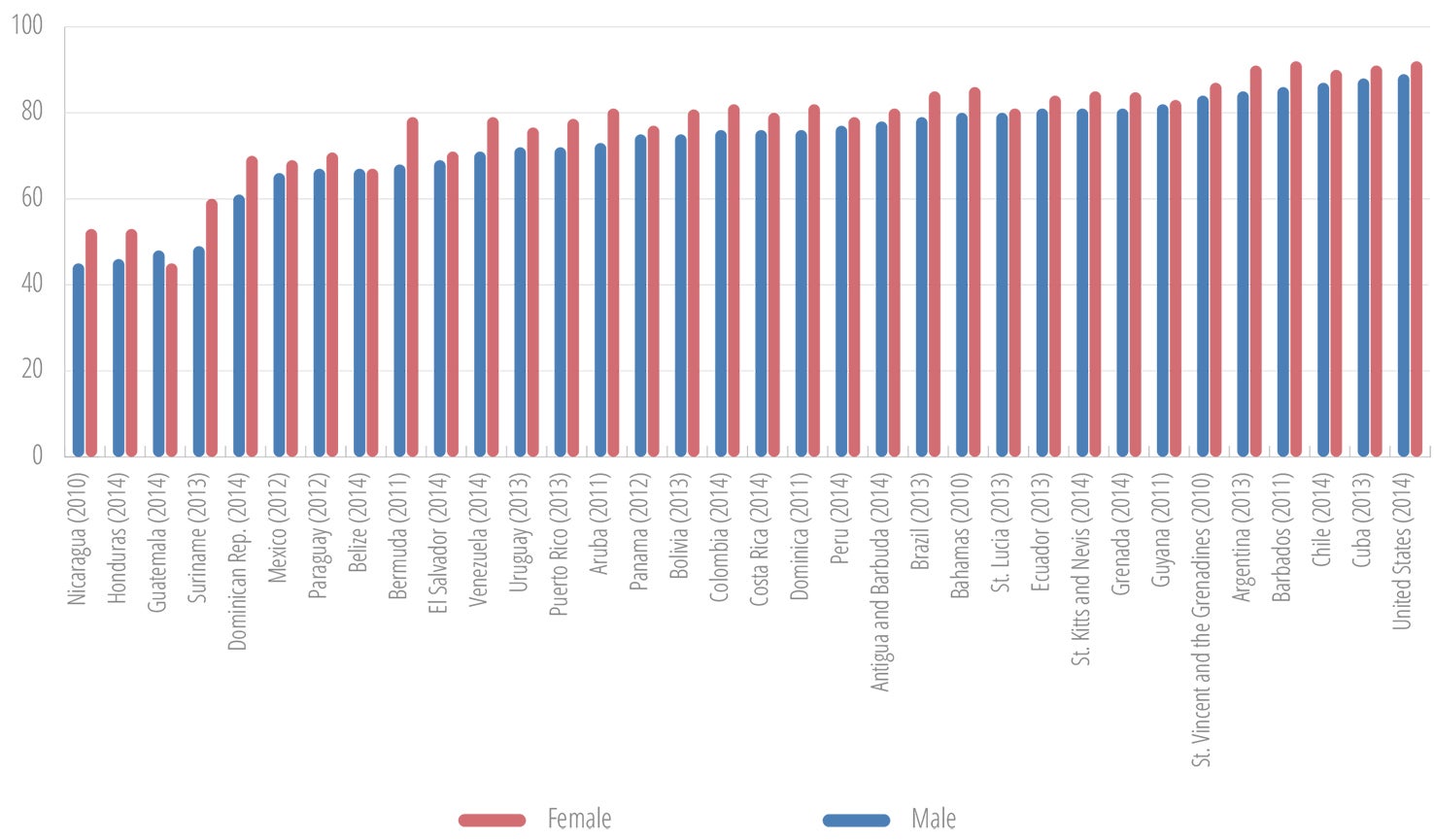
In the Americas, the literacy rate of youth (15-24 years old) is estimated at higher than 98%, with a gender parity index close to 1 (17). However, the percentage of adolescents enrolled in secondary school is significantly lower, for most countries ranging between 60% and 80%, with consistently more girls enrolled in all countries, with the exception of Guatemala and Paraguay. A few countries in the Region, including Guatemala, Honduras, Nicaragua, and Suriname, have secondary school enrollment rates below or close to 50% (Figure I.4).
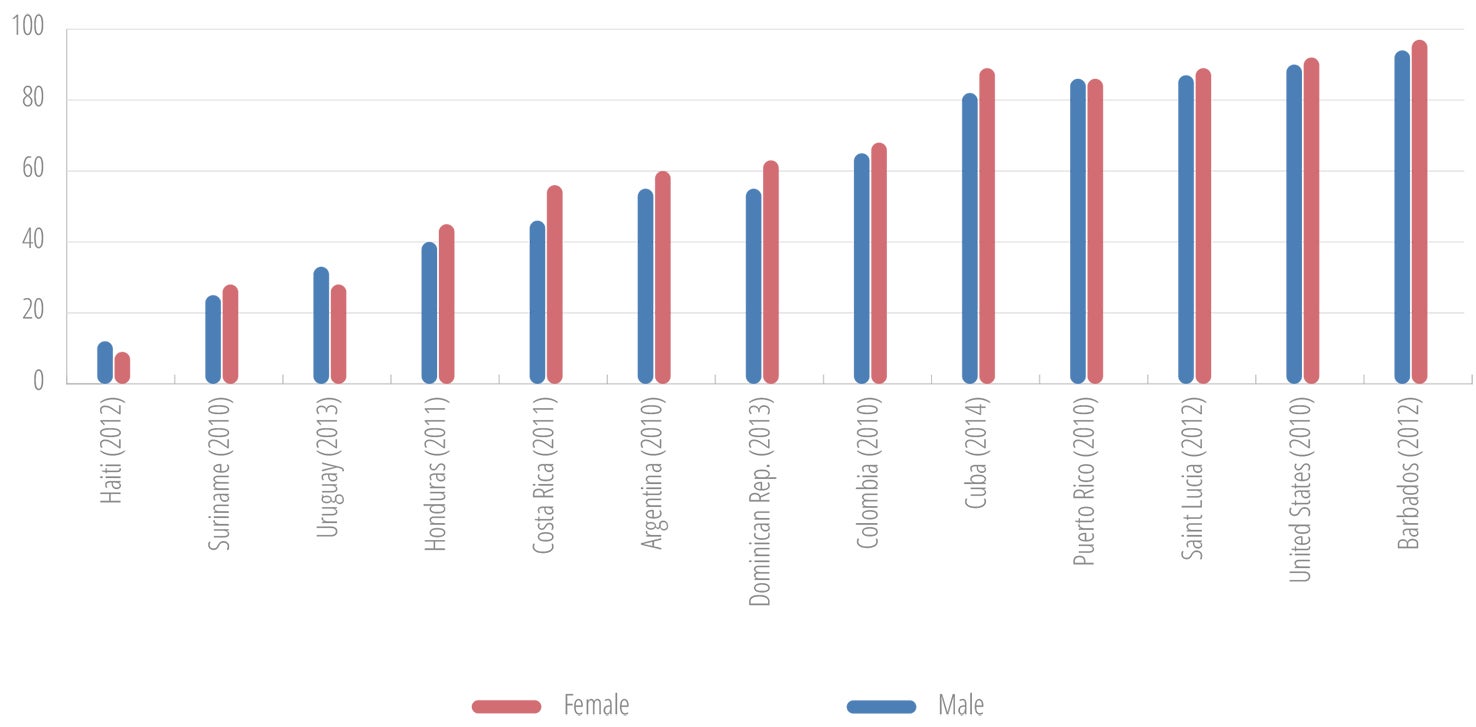
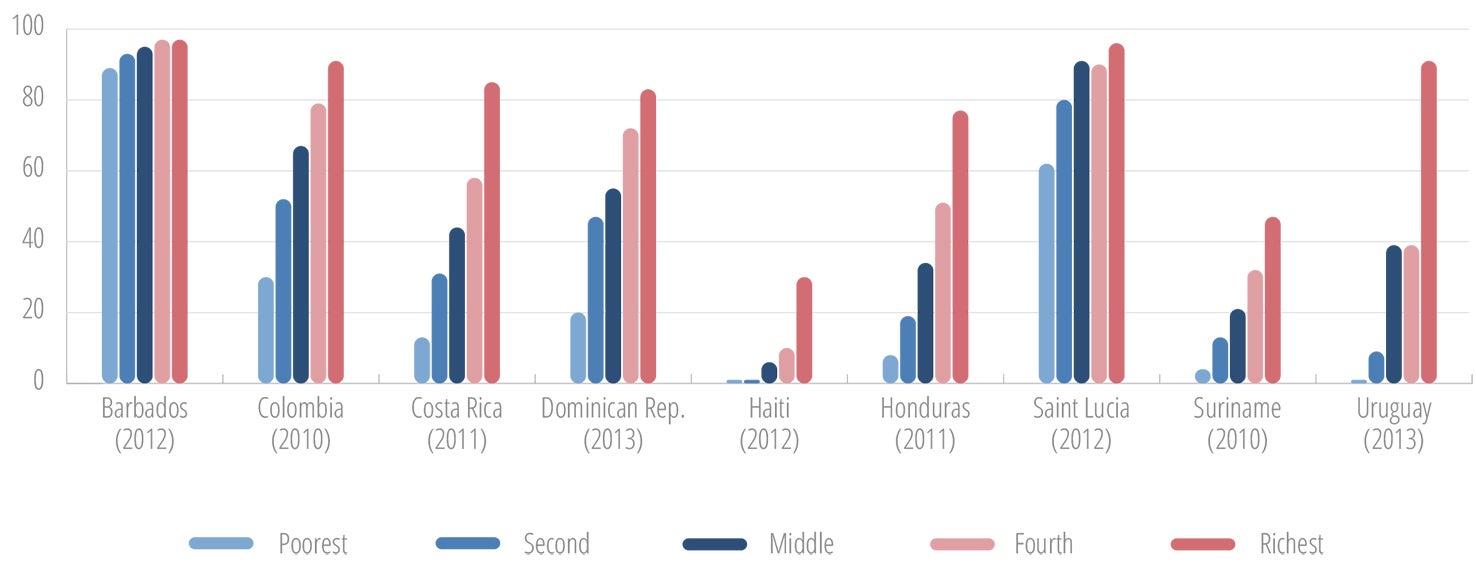
There are marked differences in educational attainment between and within countries, and between subgroups. In most countries, females slightly outperform males in the completion rate for upper secondary education (Figure I.5), and young persons from the higher wealth index quintiles have clear advantages when compared with their counterparts from lower wealth index quintiles (Figure I.6) (17).
Indigenous and rural youth are also less likely to complete secondary school than are nonindigenous persons and those living in urban settings (18).
Employment
Many persons enter the work force as adolescents, as part-time or full-time workers. Based on available information from 18 countries, the Economic Commission for Latin America and the Caribbean (ECLAC) estimates that around 76 million persons between the ages of 15 and 29 years, equaling 50% of persons in that age group, are employed in Latin America, of which 10% are both studying and working (18).
According to the International Labour Organization (ILO), not all forms of work done by young persons should be classified as child labor to be avoided. Participation by adolescents in work that does not affect their health and personal development or interfere with their schooling can potentially have a positive influence on their development and future employment opportunities (18, 19). Nevertheless, there are risks and potential negative consequences associated with early entry into the labor force, including interruption of education, difficulty in finding decent work, and decreased wages, job security, and social security coverage. Young persons who enter the work force early may end up in the informal sector in low-paying jobs, with limited opportunity for upward mobility, or even in jobs that are classified as dangerous (18-20).
The ILO defines youth unemployment as the share of the labor force ages 15-24 without work but available for and seeking employment (19). According to modeled ILO data for the period of 2015 through 2017, among world regions and subregions, Latin America and the Caribbean was expected to show the largest increase in youth unemployment over that time period, and North America was projected to have a slight decrease (Table I.2) (21). In addition to the general difficulty that young persons have in finding decent work, there are also specific groups of young people who face additional challenges in finding decent employment. This is true for those with disabilities and for young persons who face other types of exclusion, such as ethnic minorities and young persons living with HIV.
| Region/Subregion | Unemployment rate (percentage) | Unemployed youth (millions) | |||||
|---|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2015 | 2016 | 2017 | ||
| World | 12.9 | 13.1 | 13.1 | 70.5 | 71.0 | 71.0 | |
| Americas | Latin America and the Caribbean | 15.7 | 16.8 | 17.1 | 8.5 | 9.2 | 9.3 |
| North America | 11.8 | 11.5 | 11.7 | 3.0 | 2.9 | 2.9 | |
NEET: The term “NEET” refers to young persons who are not in education, employment, or training. An estimated 21% of young people in the age group 15-29 in Latin America and the Caribbean are in this category, with 76% of them female (22). Notably, despite higher secondary school enrollment and completion by females, they are disproportionately represented in the NEET category. The NEET status is concerning, because it exponentially increases the risk of social exclusion and poverty across the life course. The NEET status does not necessarily mean that these young people are not contributing to society, since many, in particular females, may be engaging in informal household-related tasks such as child care and housekeeping. This greater engagement of females in informal household tasks may partially explain why there are more females in the NEET category, while girls outperform boys in secondary school enrollment and completion rates.
Not all NEET youth remain in that position. Instead, they may be moving in and out of this status, depending on the availability of employment opportunities. An important component of national efforts to make young people thrive is the implementation of programs to keep young persons in school as long as possible and to facilitate optimal school-to-work transitions, with decent employment opportunities.

Source: (22).
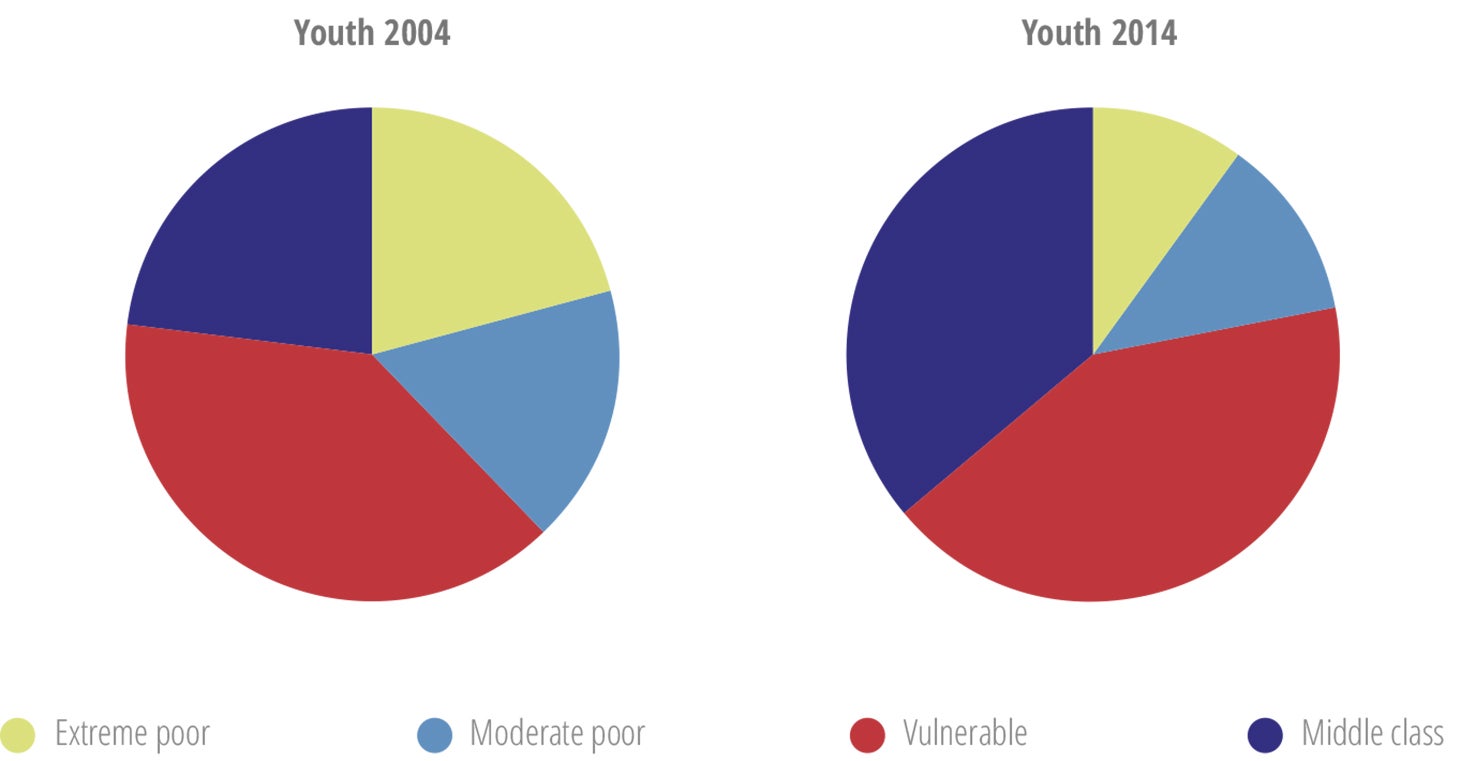
Note: Socio-economic classes are defined using the World Bank classification: “Extreme poor” = youth belonging to households with a daily per capita income lower than USD 2.50. “Moderate poor” = youth belonging to households with a daily per capita income of USD 2.50-4.00. “Vulnerable” = individuals with a daily per capita income of USD 4.00-10.00 “Middle class” = youth from households with a daily per capita income higher than USD 10.00. Poverty lines and incomes are expressed in 2005 USD PPP per day (PPP = purchasing power parity).
Poverty
In recent years, the Region has made remarkable macroeconomic progress. Over the 2004-2014 period, the income pyramid in LAC underwent a historic transformation, in which 72 million people escaped poverty and 94 million joined the middle class (23). However, the gains are not necessarily stable, and not all groups benefitted equally from this progress. An estimated 25 to 30 million people in the Region risk falling back into poverty, many of whom are youth, women, or persons of indigenous or African descent (23). From 2004 to 2014, the percentage of extremely poor and moderately poor youth aged 15-29 years has decreased, but the percentage of vulnerable youth has increased during this period (Figure I.7) (22).
Ethnicity
This determinant is highly relevant for the Americas, considering its ethnic diversity. In its policy on ethnicity and health (24), PAHO recognizes indigenous peoples, Afro-descendants, and Roma as ethnic groups that experience structural discrimination, exclusion, poverty, lack of access to basic services (such as water and sanitation), low levels of education, low rates of participation and representation in decision-making processes, and more employment in low-paying jobs (25-30).
More than 400 different indigenous groups are represented in the Americas, totaling some 45 to 48 million people (31). Around 90% of indigenous people in the Region live in just five countries: Bolivia, Guatemala, Peru, Ecuador, and Mexico (32). In Bolivia and Guatemala, the majority of the population is indigenous, 62% and 60%, respectively. In contrast, in Brazil, Paraguay, and Venezuela, the indigenous population comprises less than 3% of the total population (31, 33). In the Caribbean, Suriname and Guyana also have small indigenous populations, 2% and 10%, respectively (34).
Indigenous groups currently account for around 17% of those living in extreme poverty in Latin America, even though they represent less than 8% of the population (28). Indigenous young people tend to have lower levels of educational enrollment and attainment, as compared with their nonindigenous counterparts (35). Analysis of data from 11 Latin American countries revealed a more than 20-point illiteracy gap between indigenous and nonindigenous populations (28). As elaborated in Part II of this report, indigenous adolescents are also disproportionately affected by early pregnancy (36).
All the subregions of the Americas have large Afro-descendant populations, each with their specific historically developed population dynamics. A common theme is the subordinate place that Afro-descendant groups tend to occupy in societies (originating from the history of slavery), along with greater levels of poverty and social and political exclusion in most subregions, perhaps with the exception of the Caribbean (37). Afro-descendants may well be the most invisible and marginalized population group in Latin America, even with a population size of more than 100 million. Brazil has the largest number of Afro-descendant inhabitants, in both absolute and relative terms. Other Latin American countries with significant Afro-descendant populations include Colombia, Costa Rica, Cuba, Ecuador, Mexico, Panama, and Venezuela (37). Available data for Afro-descendants indicate lower educational achievements and greater representation in the lower wealth quintiles, as compared with other ethnic groups (37, 38).
The limited available data on the Roma population indicate that Roma households often live in extreme poverty, lacking electricity, clean water, sanitation facilities, and access to public health services (29).
Gender
Some of the key health-related patterns among young people ages 10-24 years in the Americas illustrate the critical importance of gender dynamics in this age group. The following paragraphs highlight mortality and sexual and reproductive health (SRH) of young persons as examples to illustrate the importance of gender dynamics in the health of adolescents and youth.
As detailed in Part II of this report, around 150,000 young people aged 15-24 years die each year in the Region, of which around 80% are males (39), indicating the significantly higher risk of young males to die prematurely. Nine out of 10 homicide deaths and 3 out of 4 suicide deaths in this age group are among males. In order to reduce preventable deaths among young men, in particular those due to violence, it is essential to understand the underlying factors contributing to these differences between males and females. A study conducted in Mexico, the United States, and the United Kingdom presents some key findings and considerations regarding masculinity and being a young man (Box I.1) (40).
Box I.1: The “Man Box”
A recent study (40) defined the “Man Box”—a set of socially reinforced rules about what “ real men” should do—in terms of in seven pillars: 1) self-sufficiency; 2) acting tough; 3) physical attractiveness; 4) rigid masculine gender roles; 5) heterosexuality and homophobia; 6) hypersexuality; and 7) aggression and control.
Among the study’s key findings and conclusions were:
Young men’s ideas about masculinity are strongly connected, in complex ways, with how they feel about themselves. Some men are able to reject restrictive, negative social pressures related to masculinity, but many embrace these pressures and rules, as well as the version of manhood they represent.
Young men in the Man Box, it appears, experience some reward for meeting these societal expectations. However, the Man Box also exacts a high cost in terms of mental health. It tells men they should always be tough, no matter the circumstances. It tells them to act strong even when they feel uncertain. Their bravado and outward posture that “all is fine” mask deep insecurities, depression, and frequent thoughts of suicide. Those in the Man Box are even less likely to turn to peers and friends for help when they need it.
Study results show that young men are learning to embrace emotional vulnerability, but that they most often grapple with emotions on their own or with the support of women in their lives. By and large, young men do not seek emotional support from their fathers. Fear of appearing vulnerable or gay still has a powerful influence over young men’s behaviors, particularly for men in the Man Box.
Quantitative and qualitative data underscore that the Man Box is a place of risky health behaviors, particularly alcohol abuse and dangerous driving. In all three countries, men in the Man Box are more likely than those outside of it to report regular binge drinking and recent traffic accidents.
Young men’s sense of physical attractiveness, while relatively high, still links primarily with muscle bulk and body shape, as opposed to a more inward, individual sense of confidence and attractiveness.
The Man Box is an enormously violent place, with negative repercussions for young men themselves, for young women, and for others around them:
Men inside the Man Box are dramatically more likely to both experience and perpetrate all three forms of bullying included in the study: verbal, online, and physical.
Men inside the box are also far more likely to report having perpetrated sexual harassment against a woman or girl in the last month.
The overall conclusion is that the Man Box is alive and well in Mexico, the United Kingdom, and the United States. At the same time, a majority of men interviewed support ideas of gender equality.
The harmful effects of the Man Box are severe, real, and troubling. The majority of men who adhere to the rules of the Man Box are more likely to put their health and well-being at risk, to cut themselves off from intimate friendships, to resist seeking help when they need it, to experience depression, to think frequently about ending their own life, to use violence against other young men, to experience violence, and to sexually harass women.
Breaking out of the Man Box is not something that young men can do on their own. Navigating the rewards and punishments of manhood is a real dilemma in many settings. Young men and young women, parents, educators, the media, teachers, romantic partners, and all members of society have a role to play in reinforcing positive, equitable, unrestrictive ideas of manhood.
Source: (4).
Part II also elaborates on the persistently high levels of adolescent fertility and the growing trend in pregnancies in girls under 15 years old in LAC countries. Among the underlying gendered causes of inequalities that contribute to vulnerability and risk for early pregnancy (“gender drivers”) is tolerance and acceptance of sexual and gender-based violence. These gender drivers play out at the individual, relationship, and community level, and they can be sustained in institutional or systemic responses, such as service delivery protocols, legislation, and policy frameworks (41).
There is growing recognition of the importance of engaging boys and young men in sexual and reproductive health and rights (SRHR) and gender equality, both for their own health and for the health of women and girls (42, 43). Some of the evidence for this comes from the currently ongoing Global Early Adolescent Study (GEAS), a 15-country study among adolescents aged 10-14 years on the evolving nature of gender norms and social relations. That study has found that young adolescents begin to endorse and internalize norms and values that perpetuate gender inequalities, and that parents and peers are especially central in shaping these attitudes. These results suggest that the investment in and engagement of young adolescents, in particular boys, should start early (44, 45).

Family, peers, school, community and media
It is well-established that the health and development of adolescents are profoundly affected by the relationships with parents, peers, the school and their communities (15, 16, 46). Significant associations have been found between low levels of connectedness or emotional attachment with the family, peers, school and community, and increased risk of negative health outcomes and behaviors such as anxiety, depression, suicide ideation and attempts, unsafe sex, unplanned pregnancy, and substance use (46). On the other hand, positive relationships and high levels of connectedness can promote emotional and physical well-being, and protect adolescents from engaging in behaviors that may compromise their health in the short, medium and long term.
A life course perspective on the social determinants of health recognizes the importance of time and timing in understanding how the social determinants operate at the various stages of life to influence health across the life course (3) (Figure I.8).
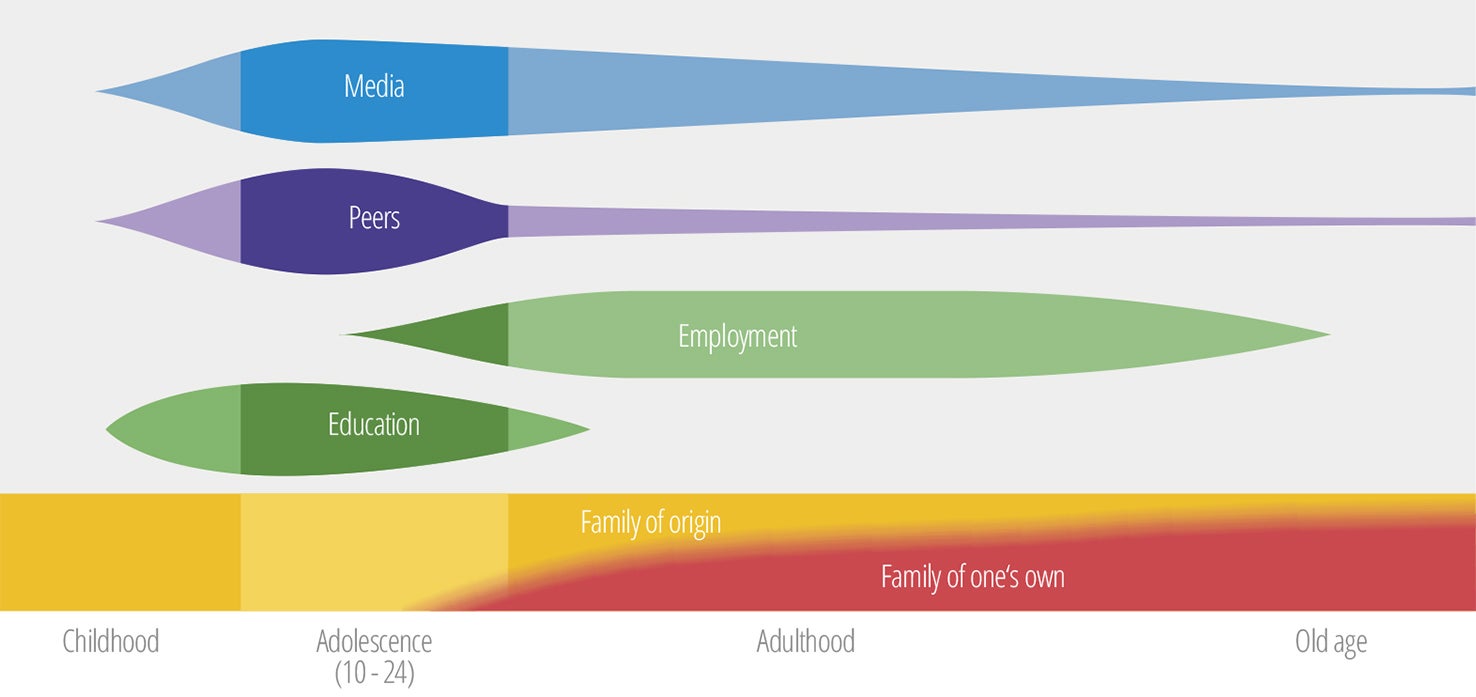
Family connectedness is among the most important factors that protect against poor health outcomes in adolescents. As illustrated in Figure I.5, the family remains a constant factor across the life course, even though over time the emphasis shifts from family of origin to one’s own family. In contrast, the influence of education and school, peers and media changes over time, and may be the strongest during adolescence (3).
The social environment may have positive, protective, or harmful effects. For instance, young people whose parents smoke or drink alcohol are more likely to engage in these behaviors (16). Similarly, strong connections with prosocial peers can support positive health, while peer engagement in harmful behaviors can contribute to adoption of these behaviors. An example of extreme negative peer influence is the involvement in youth gangs. Studies suggest that young people can be drawn to gang life in search of belonging, self-esteem and protection. Lack of supervision and limited access to after-school activities or opportunities to develop hobbies or play sports are potential risk factors for gang involvement (47).
As elaborated in the following section, the emergence of new digital technology and social media can amplify peer connections and influence in a positive as well as negative way.
I.2 Young people in the digital era
There is a marked difference between the current cohort of young people and previous generations in the place and meaning of digital technology in their daily lives. Young people are often referred to as “digital natives” because they were born after such digital technology as the Internet, cell phones, computers, Facebook, Twitter, and other social media had been introduced or were going to scale. As a result, these young people have never known a world without these media, and digital technology plays a central and ever-increasing role in their lives.
By contrast, their parents and older generations are referred to as “digital immigrants.” They generally do not have such an intuitive relationship with digital technology, and they need to make an effort to adapt to the new digital world.
The mobile phone was adopted throughout the world at a historic pace (Annex I.A). Currently, all age groups, including adolescents, rely on mobile-cellular technology for making phone calls and accessing other digital services and platforms, including the Internet and social media. Access to the Internet and utilization of digital technology are also well integrated in the Region (Table I.3).
| Indicator | Value |
|---|---|
| Proportion of individuals of all ages using the Internet in the Americas | 65.9% |
| Proportion of individuals aged 15-24 years using the Internet in the Americas | 88.4% |
| Proportion of households with Internet access in the Americas | 65.3% |
| Internet penetration rate for men in the Americas | 65.1% |
| Internet penetration rate for women in the Americas | 66.7% |
The percentages of Internet users in North America, South America, and Central America are above the global average, while the figure for the Caribbean is slightly below that average (Figure I.9).
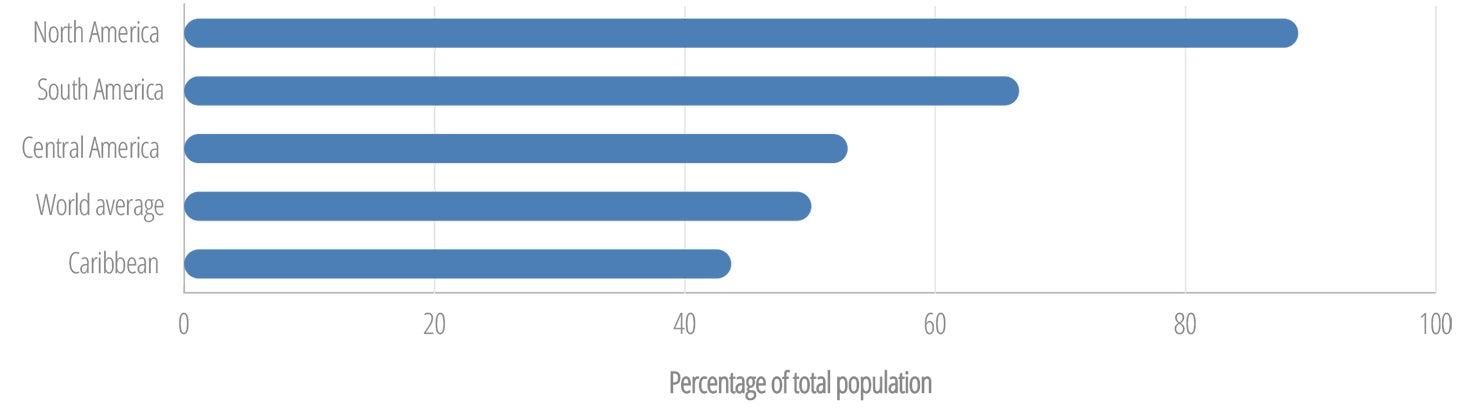
At the global level, the proportion of women using the Internet is 12% lower than the proportion of men (48). The Americas is the only region where the Internet user gender gap is inverted, with more women than men using the Internet (48).
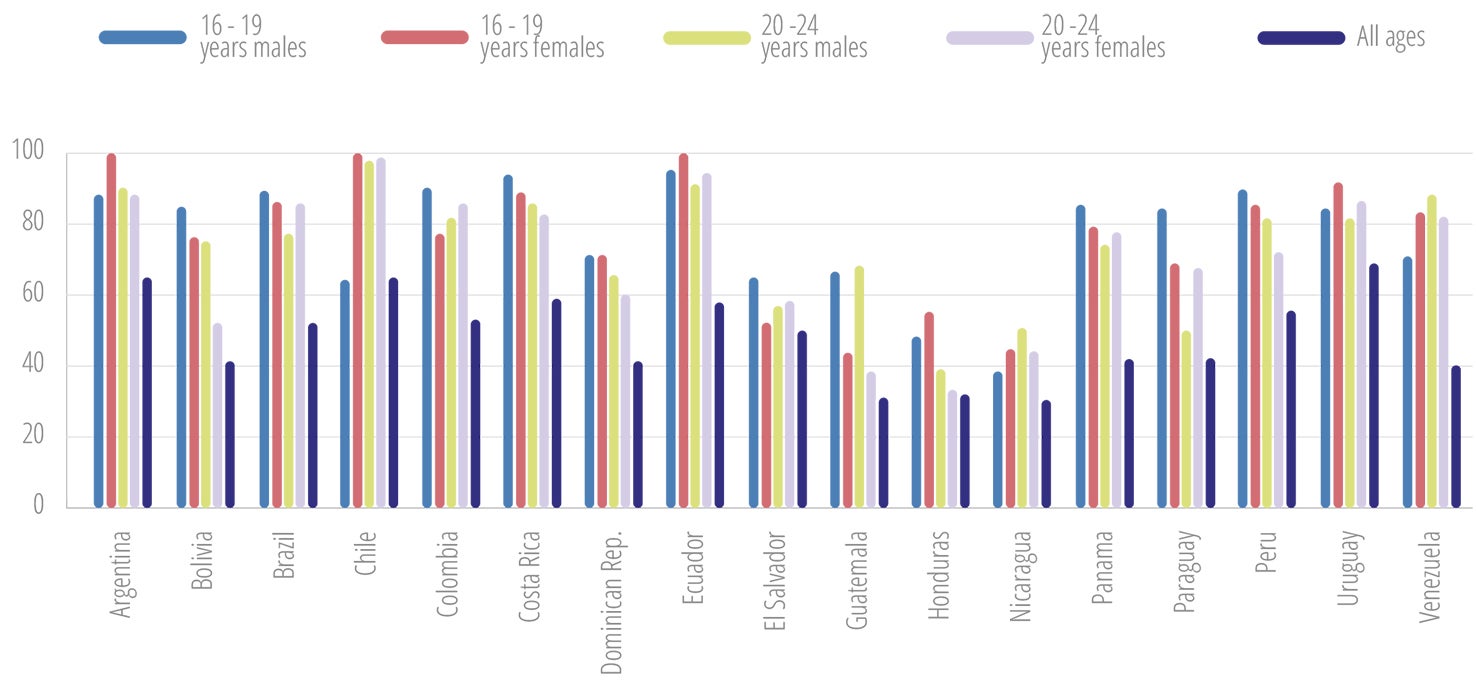
Facebook is widely used in the Region (Figure I.10 and Annex I.B). The data on Facebook use by age group clearly illustrate that young persons have a substantial lead in the use of social media.
Young people use information and communication technology in a multifunctional and integrated way. This includes doing homework, finding information, staying connected with their interests, and communicating with others. Digital technology is also increasingly used as a public health tool, to provide information and services for young persons. However, evidence regarding best practices in the use of digital technology to improve the health of young people remains limited at this time.
In addition to the benefits, there are also a range of potentially negative consequences of the high level of use and dependency of young persons on digital technology. These include excessive and compulsive use of social networking sites, dependency on and influence of virtual relationships, internet gaming, exposure to online predators, and cyberbullying. Ongoing research is needed to increase understanding of the risks and threats associated with young people’s use of digital technology, and to inform measures to protect them from these risks and threats.
PAHO conducted an in-depth literature review of 37 articles on the use of technology in adolescent health. The digital technology used in the articles included electronic TV monitoring devices, web-based interventions, mobile phone and social media interventions, and the target behaviors included weight management, smoking, alcohol consumption, mental health, sexual and reproductive health, and management of chronic conditions. Twenty-six of these articles reported positive results from the implementation of digital health technologies and techniques in adolescent health, three presented neutral results, seven presented mixed results, and one presented negative results.1 The study, which documented this negative impact, was a mobile health intervention targeting adolescents aimed at management of their diabetes.
1 Unpublished 2017 PAHO review on the impact of eHealth on adolescent health.

I.3 Adolescents and youth in situations of vulnerability
While all young people have opportunities and challenges, some groups of young people face specific circumstances—often outside of their control—that create additional layers of vulnerability and thus require specific attention. The following paragraphs highlight difficulties faced by young people with disabilities; migrant youth; young persons deprived of their liberty; lesbian, gay, bisexual, and transgender (LGBT) youth; and young people living with chronic conditions.
Young persons with disabilities: These persons encounter the same challenges as their peers do when going through puberty and growing up, but they also face the stigma and marginalization associated with living with a disability. Around the world, people with disabilities have poorer health outcomes, lower education achievements, less economic participation, and higher rates of poverty compared to people without disabilities (50).
Data on the prevalence of disability in adolescents are limited, both globally and in the Region. The available data differ substantially, depending on the definitions, age groups, and data collection methodologies used in studies. Based on the 2010 census round in the Region and national disability surveys, the prevalence of disabilities in adolescents for selected countries ranged from around 2.5% to more than 8% (Table I.4 and Table I.5).
| Country | Year of census | Prevalence (%) | |
|---|---|---|---|
| 10-14 years | 15-19 years | ||
| Argentina | 2010 | 6.0 | 5.8 |
| Aruba | 2010 | 2.8 | 3.7 |
| Bahamas | 2010 | 4.0 | 4.8 |
| Barbados | 2010 | 2.6 | 2.4 |
| Costa Rica | 2011 | 4.1 | 4.1 |
| Cuba | 2012 | 3.0 | 3.1 |
| Panama | 2010 | 6.6 | 4.9 |
| Suriname | 2012 | 3.1 | 3.3 |
Marginalization of young persons with disabilities occurs because of a lack of access to several essentials: education adapted to their type or level of disability; decent employment when they are ready to transition to the world of work; and appropriate and quality health services, including sexual and reproductive health services. Most countries lack specific legislation, strategies and resources to facilitate full and equal access to education, training, social services, rehabilitation and health services for young persons with disabilities.
In 2014, the PAHO Member States adopted the Plan of Action on Disabilities and Rehabilitation (Resolution CD53.R12) (51). With this step, the Member States recognized that disability is a public health issue, a human rights issue, and a development priority. The Member States committed to a range of actions to improve the lives and health outcomes of persons with disabilities. These included making disability a priority in their national health policies; strengthening the legal framework and regulations in the countries and their enforcement in order to protect the human rights of persons with disabilities; and improving the production, analysis, and use of disability data in national information systems.
| Country | Year of survey | Age group | Prevalence |
|---|---|---|---|
| Chile | 2015 | 2-17 years | 5.8% |
| 18-29 years | 7.1% | ||
| Dominican Republic | 2013 | 0-9 years | 7.3% |
| 10-19 years | 6.1% | ||
| El Salvador | 2015 | 0-12 years | 8.4% |
| 13-18 years | 8.0% | ||
| United States of America | 2015 | 5-15 years | 5.3% |
| 16-20 years | 5.9% |
Migrant youth: The term “migrant” refers to a range of categories of persons who move away from their habitual place of residence, including across international borders or within a State (56, 57). People can choose to migrate to seek better opportunities elsewhere, or they may be forced to move away by circumstances or forces beyond their control. Regardless of the reason for migration, migrants can face health challenges due to limited access to resources, insecurity, family separation, discrimination, and other difficulties. Circumstances of forced or irregular migration amplify the challenges and risks for the migrants (57).
The Region of the Americas has seen an increase in the number of people who have migrated across borders. That figure reached 63.7 million in 2015, of whom 808,000 were defined as refugees (58). Forced migrants within country borders accounted for an estimated 7.1 million people, of whom the majority are in Colombia (58, 59).
Young people may migrate to seek better opportunities for education and income. On the other hand, they may face unique challenges when they are forced to move with their families, move without their families, or if migrating parents leave them behind to take care of younger siblings. As refugees, young people, in particular girls, are at disproportionate risk for harm and violence, including kidnapping, physical violence, sexual harassment, and rape (60).
Because of the critical role of the social environment—including the family, peers, and the school—during adolescence, separating youth from these social settings due to migration can have irreparable consequences for their development if there are no programs and services available to fill these gaps (46, 61).
In general, policies and measures related to migration do not include provisions to address the specific challenges faced by migrant youth. For instance, without measures to legalize their status, undocumented adolescents who may have been brought into the country by their parents, remain unregistered. Without proper documentation, migrant young persons may have limited or no access to health and social services, education, and decent employment.
Young persons deprived of their liberty: Article 37 of the Convention on the Rights of the Child (CRC) states that “no child shall be deprived of his or her liberty unlawfully or arbitrarily; the arrest, detention or imprisonment of a child shall be in conformity with the law and shall be used only as a measure of last resort and for the shortest appropriate period of time; [and] every child deprived of liberty shall be treated with humanity and respect for the inherent dignity of the human person, and in a manner which takes into account the needs of persons of his or her age” (62).
Young people can be detained for a number of reasons, including administrative detention and judicial detention. Administrative detention occurs when, as the result of a decision of an executive or administrative body, a child is placed in any public or private setting from which he or she cannot leave at will (63). Minors –as defined by the law of the country– can be administratively detained or institutionalized for many reasons, including for care, protection, treatment, or illegal immigration. Judicial detention takes place when young persons are suspected or convicted of a crime, also referred to as “children in conflict with the law.”
Without entering into the many human rights and legal dimensions associated with the detention of minors, within the context of this report it is important to note that deprivation of liberty negatively affects the development of a young person. The poor juvenile court structures, poor conditions of detention centers, and lack of internal and external controls place young persons deprived of their liberty at disproportionate risk of harm. Depending on the conditions and services of the detention location, detained young persons are at increased risk for communicable disease such as tuberculosis and HIV, as well as violence, rape, and mental health problems. Youth-focused efforts must include seeking alternative measures for young persons in conflict with the law, reaching young persons with appropriate health services while detained, and, following detention, ensuring support for successful re-integration into society.
LGBT adolescents and youth: In September 2013, the PAHO Member States adopted a landmark resolution addressing the causes of disparities in health service access and utilization for LGBT persons (64). The resolution acknowledges the political, sociocultural, and historic barriers and violence that LGBT persons face in the community and when accessing health services. It also urged Member States to work to promote the delivery of health services to all people, with full respect for human dignity and health rights, taking into account the diversity of gender expression and gender identity.
The limited available data on LGBT adolescents and youth confirms their disproportionate risks and vulnerabilities (65-68). According to data from the 2015 national Youth Risk Behavior Survey (YRBS), lesbian, gay, and bisexual (LGB) students in the United States were 140% more likely (12% vs. 5%) to not go to school at least one day during the 30 days prior to the survey because of safety concerns, as compared with heterosexual students. LGBT youth were also at greater risk for depression, suicide, substance use, and risky sexual behaviors. Nearly one-third (29%) of LGB youth had attempted suicide at least once in the prior year, as compared to 6% of heterosexual youth.
A survey with more than 10,000 adolescents aged 13-17 years from a wide range of social, cultural, and ethnic backgrounds in the United States found that many LGBT adolescents are profoundly disconnected from their communities. Those LGBT adolescents also believe to a greater extent than their non-LGBT peers do that they must leave their communities in order to make their hopes and dreams come true. When given an opportunity to describe their most important problem or the one thing in their lives they would like to change, LGBT adolescents and their non-LGBT peers had different experiences and priorities. The non-LGBT adolescents listed exams/grades, college/career, and financial pressures related to college and jobs as their most important problems. In contrast, LGBT adolescents described their most important challenges as being directly related to their identity as LGBT, such as nonaccepting families, bullying, and fear of being open or out (69).
Young persons living with chronic conditions: These young persons have the same developmental issues, challenges, and needs as their peers, in addition to dealing with their chronic condition. While information is limited on the burden of chronic conditions among young persons in the Region, the available data suggest a significant burden, ranging from respiratory conditions such as asthma to diabetes, cancers, epilepsy, skin and musculoskeletal conditions, and HIV. Each year in the Americas, more than 600 adolescents aged 10-19 die from epilepsy and more than 1,000 from diabetes and heart disease (39). In an analysis of data from the 2015 Global Burden of Disease (GBD) study conducted for PAHO by the Institute for Health Metrics and Evaluation (IHME), skin diseases and asthma were among the top 3 risk factors for disability-adjusted life years (DALYs) in LAC for the age group 10-14 years, and in the top 10 for the age group 15-19 years.
Chronic conditions can be challenging in any stage of life, but the physiological and psychosocial dimensions of adolescence bring added difficulties. Chronic illness during puberty may cause temporary or permanent delays in growth and development, as well as impair the psychosocial development of the young person (70, 71). Some studies have found that young persons with chronic conditions are at higher risk for depression and self-harm, including suicidal ideation and attempts (72).
Another important aspect of chronic disease management in adolescents is the effective transfer of the adolescent from pediatric to adult care. This can take place in early adolescence, depending on the legislation and the health system policies and practices in the country. Careful consideration and attention must be given to facilitate an effective transition, ensuring appropriate support for the adolescent (73).
Conclusion
This profile of young people in the Americas sketches a portrait of opportunity and challenges. The presence of a historically large cohort of young people in the Region provides the opportunity for rapid socio-economic growth, if strategic investments are made in the health and development of young people. On the other hand, secondary education completion rates among young people in the Region are low, below 50% in many countries, which reduces the chances for young people to gain decent employment as they transition into adulthood. Other challenges include the disproportionate burden of poverty among young persons, youth unemployment, and significant numbers of young people who are neither in school, nor employed. The profile also highlights groups of young people who are living in specific situations of vulnerability, such as young people with disabilities, LGBT, indigenous and Afro-descendant youth. The potential to reap the benefits from the demographic dividend, and to achieve de SDGs without leaving any young person behind, will require comprehensive, intersectoral and pro-equity actions aimed at empowerment of young people, addressing the social determinants of their health, and maximizing the positive benefits of the family, the school, the community, social media, and other social platforms, to create an environment in which every young person can thrive.